

The Centers for Medicare & Medicaid Services (CMS) has published the Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers rule. Tipping the scales at 651 pages there is no doubt it is a federal document. I was thinking what would have happened if my mom gave me a rule 651 pages long….I would still be grounded.
In reading through the estimated hours predicted for various facilities to develop the required documents it makes me question what the intent of the rule really is. I have no doubt organizations will come up with written documentation to meet the rule so they are in compliance. I also have little doubt that the documents produced in many cases will not actually enhance preparedness in the community.
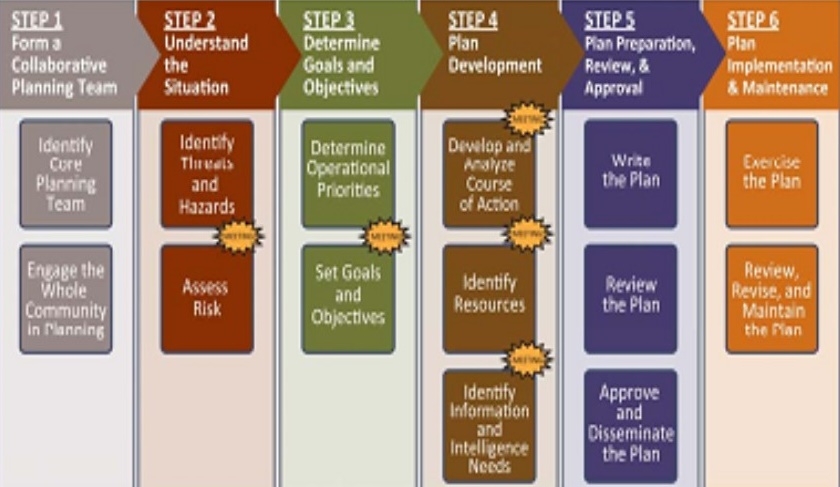 This chart outlines the FEMA recommended process to follow in developing a plan (also listed in the rule as a helpful reference). If we compare the chart with the anticipated body of planning work to accomplish to meet the new rule it does not really match up well.
This chart outlines the FEMA recommended process to follow in developing a plan (also listed in the rule as a helpful reference). If we compare the chart with the anticipated body of planning work to accomplish to meet the new rule it does not really match up well.
On the other hand I would look at this as an opportunity to boil the 651 pages down to what is necessary and more importantly what makes sense in enhancing preparedness of an organization among the whole community. In my experience there is an inverse relationship between the thickness of an organization’s (state and federal government included) plans, policies and procedures and their ability to actually implement them. It is possible to over plan and that should be avoided. In the CMS rule they point out four core elements to focus on. They are:
- Risk Assessment and Emergency Planning
- Policies and Procedures
- Communication Plan
- Training and Testing
Over the years one of the most common reasons I heard why emergency preparedness programs were disliked in healthcare facilities is that the training and exercises were so disruptive of daily operations. No one objected to one poor soul writing a plan to make them “compliant”, but the issues started when the author actually tried to implement change and ensure competency. The reality is that a well designed preparedness program and sound understanding of the Hospital Incident Command System (HICS) can actually simplify life within your organization. Both on a day to day basis and when emergencies arise. My suggested keys to building a successful program are:
- Implementable Planning – Boiler-plate plans are going to be popping up and tempting many organizations to make them “CMS compliant” yet they are seldom a good fit for any facility. Many consulting firms love them because they are easy to develop and therefore profitable to sell. They may allow you to check the box necessary to meet a grant deliverable but they will most likely fail in a real event. Developing plans that actually work may take more up front effort but make your life much easier in managing the event. Keep in mind after an event you will be judged based on your plans, polices and procedures and training records. If you can’t actually accomplish something you’ve documented in your plan you are setting yourself up for misery and liability.
- Practical Training – I consider education to be a key factor in how people will perform under stress. Canned courses are like boiler-plate plans. Usually longer than they need to be and a good portion of the content is is irrelevant to your organization or performance expectations. I am often accused during my courses of making people think. It’s not rocket science stuff. I simply give them material which is relevant to their current situation, aligns with organizational expectations and is focused on need to know material.
- Realistic Exercising – Properly designed and facilitated, exercising is where we can evaluate the results of our planning and training components. Part of exercising is the evaluation component and developing a Plan of Improvement. These findings go into the next evolution of planning and training effort. Exercising without incorporating what we have learned is a waste of effort and resources. For additional information on ideas for a good exercise program click on the link.
While the intent of the ruling is to raise the bar of emergency preparedness in individual facilities, the final outcome should be a better prepared community. You may be able to find assistance from other members of the healthcare or emergency management organizations in your area. Regardless of the route you take to meet the ruling, internal work effort, other community partner agencies or a consultant, make sure your preparedness program passes this common sense test.
- If a predictable event(contained in your Hazard Vulnerability Analysis) occurs, does your staff understand their role in ensuring the safety of all staff, clients and visitors? This includes staff on campus as well as working at remote locations.
- Does your organization utilize the HICS to manage events and trained staff have demonstrated competency in its use? If efficiency in operations and effectiveness in outcomes is desired, spend time learning how to use the HICS and not just spell it out.
- Has your organization developed sufficient documentation (plans, polices, procedures, initial Incident Action Plans) for staff to understand how they will provide for the continuity of patient care in emergencies? This may require coordination with other community partners as necessary and appropriate.
- Is organizational leadership 100% engaged in the preparedness process?
I would love to hear from organizations and how they are intending to proceed in order to meet the intent of the rule.


Jan,
A good overview of the new CMS rule. I reviewed the highlights last week and agree that the document is daunting. FEMA has learned through the years that documents can’t be digested and guidance can’t be followed if they produce things that long and detailed. Obviously the intent is sound, as is their overall guidance, but implementation is where we will see problems, especially as people scramble to meet the requirements. All your guidance, as usual, is 100% spot on!
Tim
The reality is that even with a plan and even if there is a drill, when the disaster happens the people who drilled will all be off duty and unavailable, so it better be a real simple plan that can be explained in three minutes or less to the new crew who just started working in your facility last week and happen to be the ones on site.
Jan, as usual, your comments are excellent. But, I wonder if you could give a brief “for instance” of how an “average Joe or Jane Emergency Coordinator” might go about making things simple and relevant? Because I think Barbara’s remarks are also sound–if they’re not on duty, then they simply “forgot” the plan, because it was too large and complicated to remember!
First off Jeff I would say it is not an easy task for most persons tasked with emergency preparedness in healthcare to strike a balance easily. Many of them are wearing multiple hats and emergency preparedness as a duty-as-assigned or as I discovered in several regional assessments, typically less than < 0.25 FTE of time. The "plan" needs to be compliant but this can also be achieved with some innovation if you're willing to develop a matrix which indicates where they can find their standards in an unconventional format. So long as the EOP says we will use HICS I am halfway there as now I have a tool designed to manage events regardless of discipline, hazard or function. I work with many clients to build their library of Incident Action Plans which can be found here under my services and courses tab. By giving your personnel a chance to “war-game” events in your HVA, you give them a tool to get them started for the first 12 hours, open up your Command Center, utilize HICS and start building out your next IAP and so on and so on.
Great read here at a colleagues site which speaks to the role coalitions could play. Have a read. http://www.linkedin.com/redir/redirect?url=http%3A%2F%2Fbit%2Ely%2FCPR160916&urlhash=tjDK&_t=tracking_anet
Implementation is the key component. Often this is misunderstood as following what is written instead of following what is known during the moment. There is the constant challenge of managing EM spontaneous behaviors that on the surface appear sound during the moment of crisis. The IAP is best implemented when the members of the organization understand why, who and how to get resources in the right places at the right time.
IAPs require flexibility and participants need to understand the importance of disaster behavior psychology. Dennis Mileti’s “Disaster by Design” research into the mind of survivors is a must read for everyone responsible for designing an IAP.
As an experienced emergency manager, so much of my time is wasted managing the questions and donations from well meaning personnel that are unfamiliar with the key players and response functions of our organization. People will behave in the future as in the past. For example someone will again call their brother in law who has a pick-up truck because they always do this during family emergencies, then they go to the local hardware store for an extra generator with the expectation that we or FEMA will reimburse the time, gas, etc.
Another example of EM plan implementation that concerns my peace of mind is how to mitigate “friendly fire” survivor rescue during active shooter scenarios. Something the media has yet to discuss because revealing a motive sells more ad space.
Is anyone working on plans for recovering survivors safely without endangering response personnel? At the present everyone is suspected to be involved as a shooter, especially when they have a right to carry permit and have discharged their weapon during the active shooter stand-off.
One thing I leaned working with the Oregon State Police SWAT as a tactical paramedic is that adding more guns to a scene by well-meaning lay persons does not make the scene safer for anyone. There are procedures that can make such situations safer but it is unlikely in most active shooter situations that any conversation or joint training will have taken place and tragedies can be expected to occur.