

I wanted to give the Medical Rapid Response Teams (MRRTs) a taste of what their mission could be like if they were flown into a coastal community and tasked with establishing a medical presence. To give them background they had the opportunity to attend my Ground Truth presentation, backed-up by the local Emergency Manager in case I said something they disagreed with.
In this presentation they were given a graphic picture of what it will look like in coastal communities across the west coast which are in the tsunami inundation zone. My research included speaking with an American school teacher working in Japan who was in a coastal community hit by the 2011 tsunami. Nothing like hearing it from someone who has been there, done that.
The situation the MRRTs faced in the night exercise was as follows. It’s 48 hours post Cascadia. A USCG helicopter returning to base for refueling notices a light source in a small devastated community along the coast. 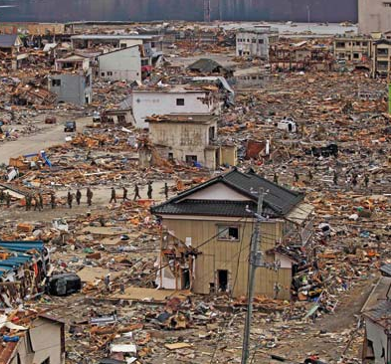 No one has been to this site due to it’s isolated location, total destruction of ground access routes and limited air assets. A rescue swimmer is lowered. He does a quick recon and is hoisted back aboard the helicopter. They report in that they saw several hundred survivors, many with medical problems who have been living in the shells of buildings still standing. One survivor in a volunteer EMT who has been doing what they can with no supplies.
No one has been to this site due to it’s isolated location, total destruction of ground access routes and limited air assets. A rescue swimmer is lowered. He does a quick recon and is hoisted back aboard the helicopter. They report in that they saw several hundred survivors, many with medical problems who have been living in the shells of buildings still standing. One survivor in a volunteer EMT who has been doing what they can with no supplies.
The county EOC is notified and they in turn contact the Medical Rapid Response Team (MRRT) Command and task them with the following. Hike (no air assets available to get them closer) from their current staging area to the location and report back the following by 2200 hours. Number of survivors, count by triage categories and immediate resource needs. The team(s) should anticipate being self-sufficient for a minimum of 72 hours before they can expect additional assets necessary to establish a more robust Casualty Collection Point (CCP) in the community.
 The exercise venue is a training village with 20-30 structures. 250 patients are scattered throughout the buildings. After the teams have been on location for one hour they get Intel from a role-player that half a mile away are roughly 50 survivors, many of them injured from a local school that collapsed.
The exercise venue is a training village with 20-30 structures. 250 patients are scattered throughout the buildings. After the teams have been on location for one hour they get Intel from a role-player that half a mile away are roughly 50 survivors, many of them injured from a local school that collapsed.
The nine MRRTs are faced with a 300 patient MCI in essence. Staged patient triage categories are consistent with data from the 2011 Japan event:
- 63.1% (green, ambulatory)
- 27.1% (yellow, serious injury)
- 7.7% (red, life-threatening conditions)
- 2.0% (black, death).
Shortly before the exercise was to be called, MRRT Command was notified that one aircraft was inbound to the site and could take eight patients. They should not expect any other air evacuations for 48 hours and the aircraft would be on target in 15 minutes. Command was tasked to determine which eight patients of the 300 survivors would be flown out. Difficult choices needed to be made in a very short period of time.
This last task lent itself to a great team exercise the next morning. Each of the nine MRRTs was given a packet of 10 patient descriptions and each packet was different. Their task was to reach consensus on which one of the ten they wanted to put on the evacuation a helicopter, based on the exercise scenario the previous evening. They had 15 minutes to make their decision and a spokesperson was to meet me in the front of the classroom.
After the time was up, each spokesperson had one minute to make their case in front of the class on which patient should go and why. After they all had briefed I gave them one last task. Each team had the one patient they wanted to fly out, but there were nine teams and only room for eight patients. They now had one minute to reach consensus who was left behind and why.
As the aircraft lifts off with eight patients out of 300 survivors, many of the remaining requiring more definitive care than the teams could offer, we have to call that a win. It won’t be business as usual, there is no fast arriving cavalry. Patients will survive based upon the ability of MRRT personnel to apply innovation in treatment modalities and the preparedness of each team member to function in this type of environment.
If you’re interested in exploring enhancing your next field exercise or want to talk about planning assistance for your at risk community or agency, contact me at abetteremergency@gmail.com


Leave A Comment